Bulimia Nervosa
1. Overview
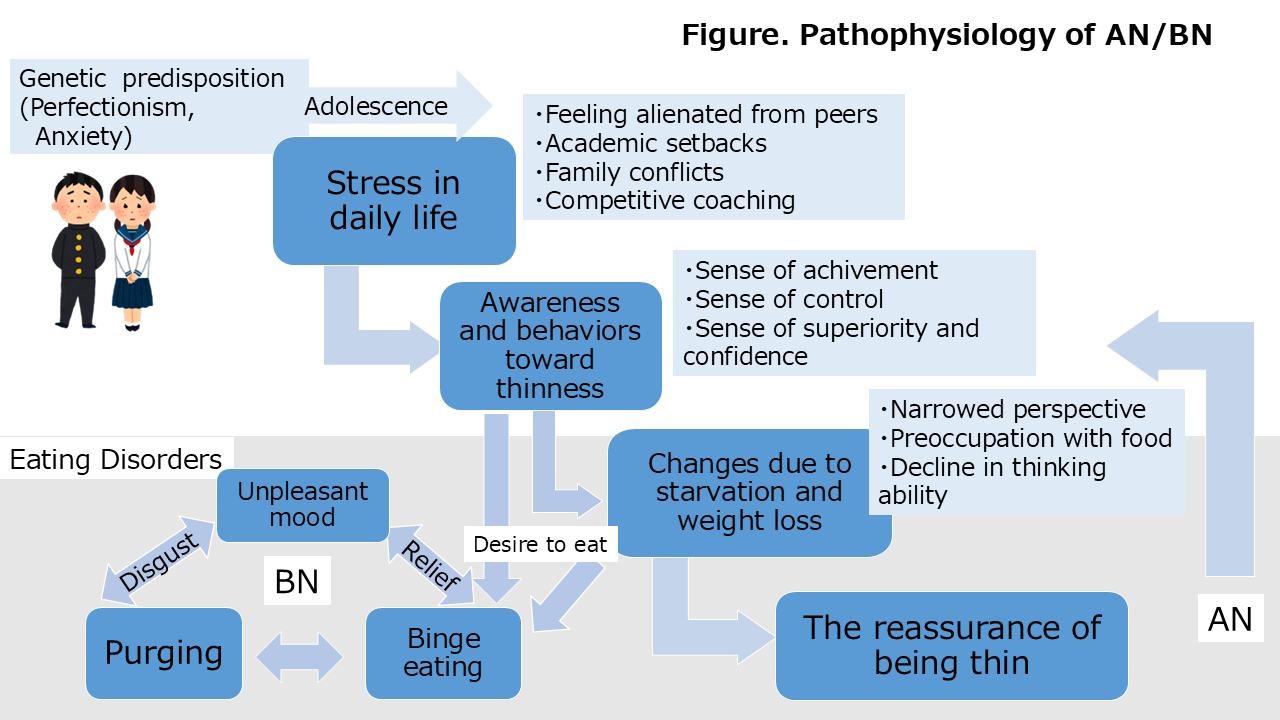
Bulimia nervosa (BN) and AN are the primary types of eating disorders. The core psychopathology in AN and BN is the “excessive coupling of self-evaluation with the perceived ability to control weight and body shape,” in which weight and body shape exert an excessive influence on the patient’s self-evaluation. Consequently, AN and BN involve a desire to be thin, fear of weight gain, and body image disturbance. However, BN is defined by binge eating and compensatory behaviors (self-induced vomiting and laxative/diuretic abuse) as abnormal eating patterns, occurring alongside a weight within the normal range. If the patient is underweight, the condition is classified as the binge-eating/purging type of AN. A lifetime prevalence has been reported at 1.3% among females teens and 0.5% among male teens aged 13–18 years. However, many cases do not lead to medical consultation, as because the body weight remains within the normal range.
2. Symptoms and diagnosis
The prepubertal onset of BN is rare; it usually begins after the onset of puberty, often in the course of dietary restriction. Binge eating in BN involves consuming large amounts of food within a short period (usually within 2 h) with a sense of loss of control over eating. Individuals often binge to relieve stress, followed by compensatory behaviors to prevent weight gain. Self-induced vomiting, sometimes aided by fingers or a hose, is the most common compensatory behavior, and over-the-counter laxative abuse is also common. Feelings of shame of the abnormal eating behavior and loss of control contribute to low self-esteem and depression. This unpleasant mood can reinforce the cycle of binge eating and compensatory behaviors (Figure). A diagnosis is made when binge eating and compensatory behaviors occur at least once a week on average over 3 months, accompanied by preoccupation with weight and body shape, indicating the need for treatment.
3. Complications and comorbidities
Physical complications:
With repeated vomiting, the salivary glands may swell, and gastric acid can erode the teeth, leading to dental caries. Binge eating can result in gastric dilation or, in severe cases, perforation. Vomiting may also cause reflux esophagitis. Furthermore, vomiting and laxative abuse can lead to hypokalemia, which may precipitate life-threatening arrhythmias. Therefore, even when body weight remains within the normal range, laboratory testing and electrocardiography are essential.
Psychiatric comorbidities:
BN is often associated with psychiatric disorders. The prevalence of depressive disorders, anxiety disorders (including social anxiety disorder), and personality disorders is high. The risk of suicide is high, as in AN; approximately one-quarter to one-third of individuals with BN have a history of suicidal ideation or suicide attempts.
4. Treatment
Evidence-based treatments for BN in children and adolescents include family-based therapy, CBT, and guided self-help approaches targeting BN.
Binge eating and compensatory behaviors often follow a chronic course; thus, the goal of treatment is not simply to eliminate abnormal eating behaviors but to help patients establish regular eating and lifestyle patterns and restore a sense of control over their behavior.
In outpatient settings, this typically involves keeping records of daily routines to identify triggers for binge eating and compensatory behaviors (self-monitoring) and collaboratively developing coping strategies (control). In Japan, no pharmacological treatments are officially approved for eating disorders; however, selective serotonin reuptake inhibitors (SSRIs) may be prescribed to address comorbid depressive or anxiety symptoms. Caution is required, as most SSRIs are not approved for use in pediatric populations.
5. Course
In BN, symptoms often persist for several years. The clinical course may be chronic or intermittent, with periods of remission alternating with recurrences. Sustained remission lasting for more than 1 year is considered associated with better long-term outcomes.
OTANI, Ryoko
Oji clinic Division of Medicine the Japanese Association on Intellectual and Developmental Disorders